Orthotropics is a growth guidance philosophy that believes proper body posture, resting oral posture, swallowing and nasal breathing patterns allows the tongue to be the conductor in developing the down and forward growth of the face. This is to guide the expansion of the jaws, facial and cranial bones and airway to its most ideal form. If function and growth were ideal, you would achieve straight teeth and room for all 32 teeth as a byproduct. The challenge in this day and age is to have ideal growth happen naturally. We feel the reason in large part is due to our current lifestyle. From the health of the mother during pregnancy, to the way we birth, what we eat, the consistency of our foods, our technology (that has impacted our sleep quality), our medications, our posture, to our diet (GMO's, organics, supplements, processed foods, etc…), how we live today is so different compared to the past. Let's discuss posture. One has to really fight for good posture. We may sit at our job all day hunched over a computer. Our children sit hunched over at their desk, then in front of the television and computer. Poor body posture will encourage poor oral posture and tongue function. Biobloc and ADAPT, ALF, and Crozat appliances and Myofunctional Therapy can help address proper horizontal, down and forward growth but in different ways.
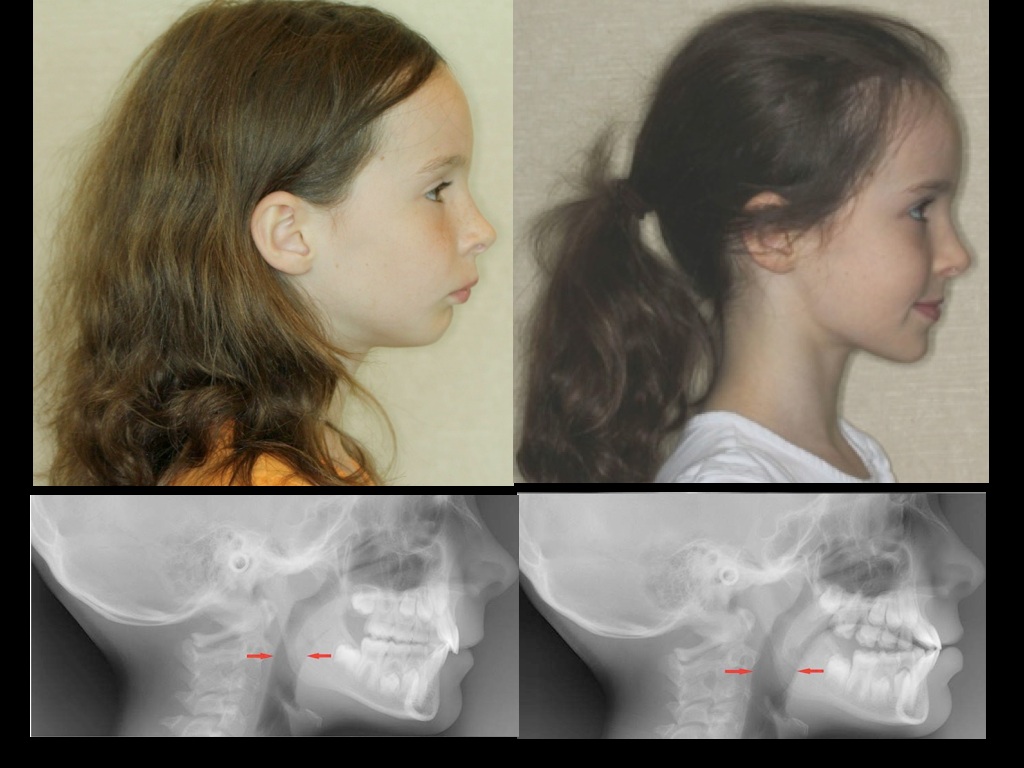
Biobloc patient, before and after.
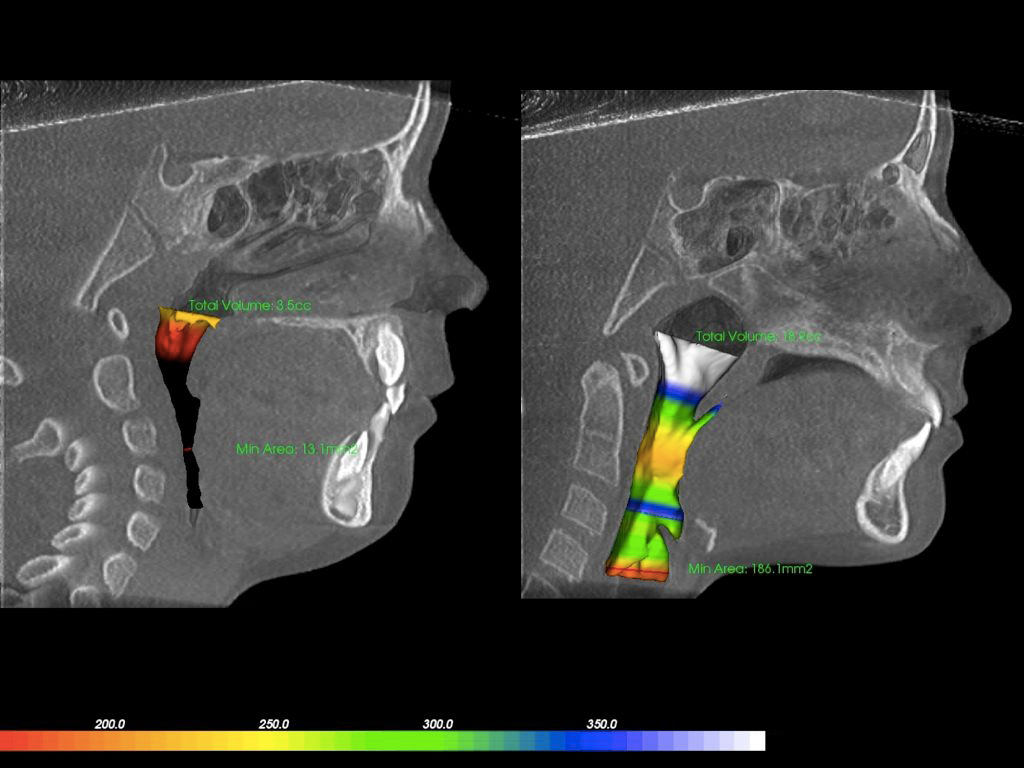
This is a six-year-old girl who completed Biobloc Orthotropics. Notice the development of the midface (including the sinus area) and the forward development of the upper and lower jaw allowing for a much larger airway (in colors). We feel this enables the child to correct her posture. In the left photo, if the child were to correct her posture, the airway would have gone to zero. In other words bad posture may be a compensation for a small airway
Part 1 in this treatment is defined by semi-rapid horizontal expansion and forward expansion to normalize the Mew line, usually leading to a large overjet to make room for the mandible to come forward. The average time for Part 1 is 4-6 months. Part 2 is defined by wearing the Biobloc/ADAPT to position the mandible in the forward position and close the overjet. The time spent in Part 2 is variable because wearing it properly requires patient compliance. The fastest we have seen in completing Part 2 is 4 months. Having a non-compliant or unmotivated patient is a good reason not to choose this method. The biggest advantage of this method is that it has the ability to make the most progress under the least amount of time, creating dramatic changes in the dentition, the face and airway. You may consider this option over others if your child has signs and symptoms such as sleep apnea, constant illness, or is older as he or she has less time left to grow. In addition, if your child has a large Mew line or is far off of the Bolton Norm, Biobloc Orthotropics give us the highest potential of getting those indicators back to ideal.
This methodology was invented by Darick Nordstrom, DDS, with the input from a Cranial-Sacral Osteopath, out of the concern that introducing orthodontic forces could be harmful to the individual. What makes ALF unique is not just the design, but also the type and thickness of the wire of the appliance. By itself, the wire is so thin that moving a tooth may be challenging. The actual way it works is also challenging to describe. We explain that the ALF behaves like a surrogate tongue. The proper place for the tongue is at the roof of the mouth. When children and adults have open mouth posture with the tongue on the floor of the mouth, the ALF helps to resist the retraction forces of the facial muscles pushing inward. Secondly, the design of the ALF attracts the tongue to push against it, encouraging the tongue to do what it was meant to do. The wire is so light and flimsy, it allows the tongue to push through the ALF and be a part of the actual expansion process. The tongue can overpower the ALF, expanding the palate laterally and encouraging forward growth. Adjusting the ALF is minimal (0.25mm at the center u loop and/or posterior loops). The main reason for adjusting the ALF is to stimulate the periodontal ligament (PDL) for growth potential. In fact, over-adjusting the ALF may result in no movement of the teeth at all. It is believed that the tongue is very strong and can move structure better than wires or any expander. Not only is the tongue incredibly powerful, but it also contacts the palate and exerts a symmetrical, intermittent and physiological force better than any expander available.
ALF Case #1
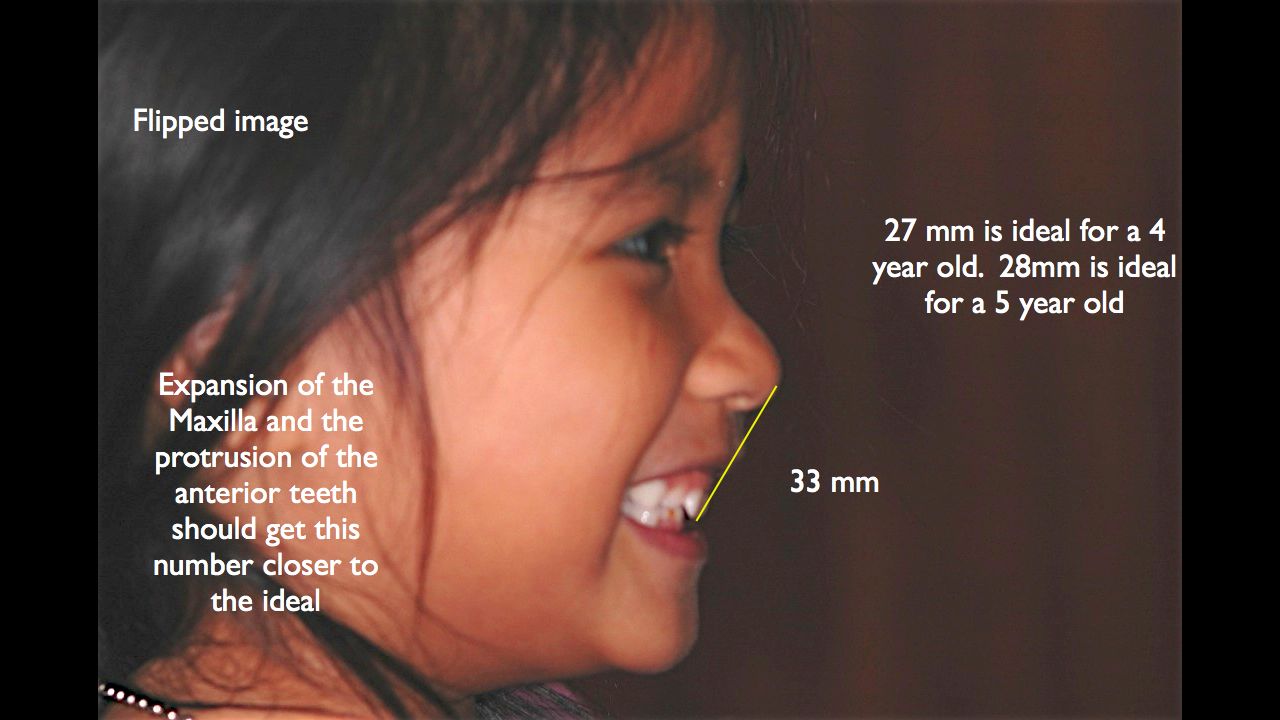
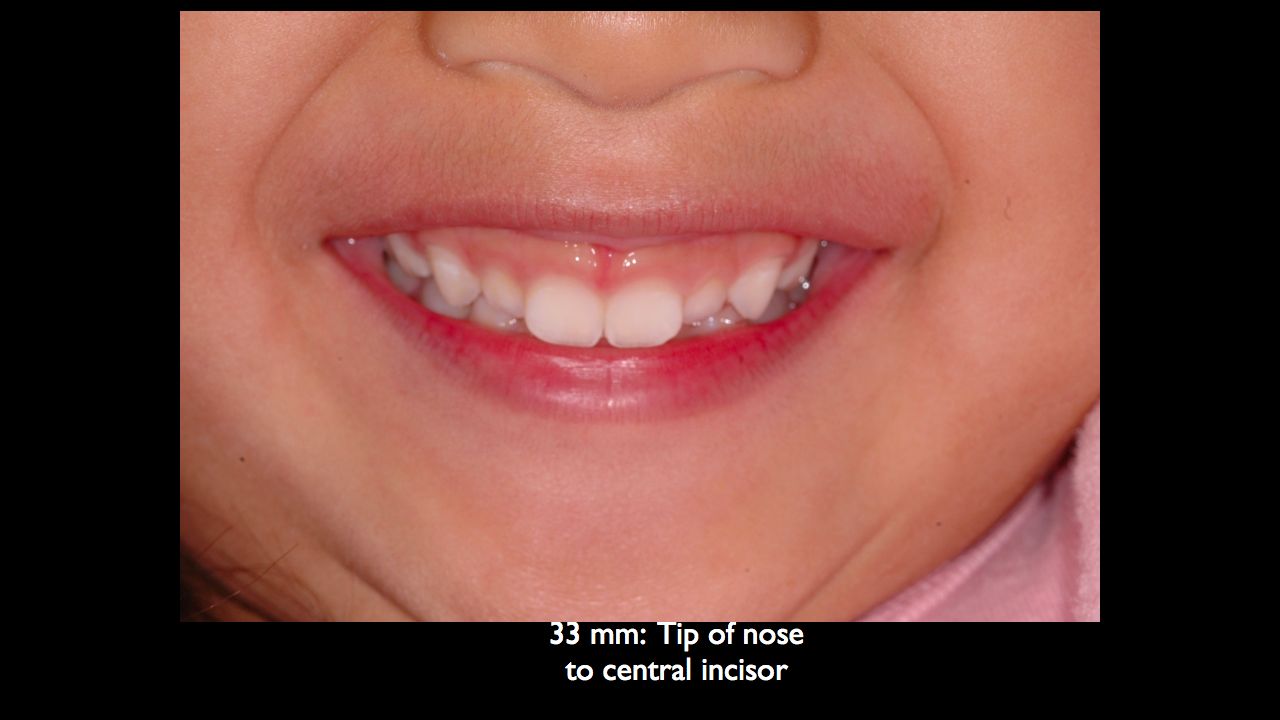
4 -yr old boy. Goal was to correct the crossbite on the patients right side. In addition to reduce his allergy sympotoms, clenching and grinding, and improve his sleep quality. Our concern in treating for the crossbite early is because we want the child to grow asymmetrically. Most crossbites at this age is in large part to deflection of poor contacts from upper and lower teeth which can easily be corrected.
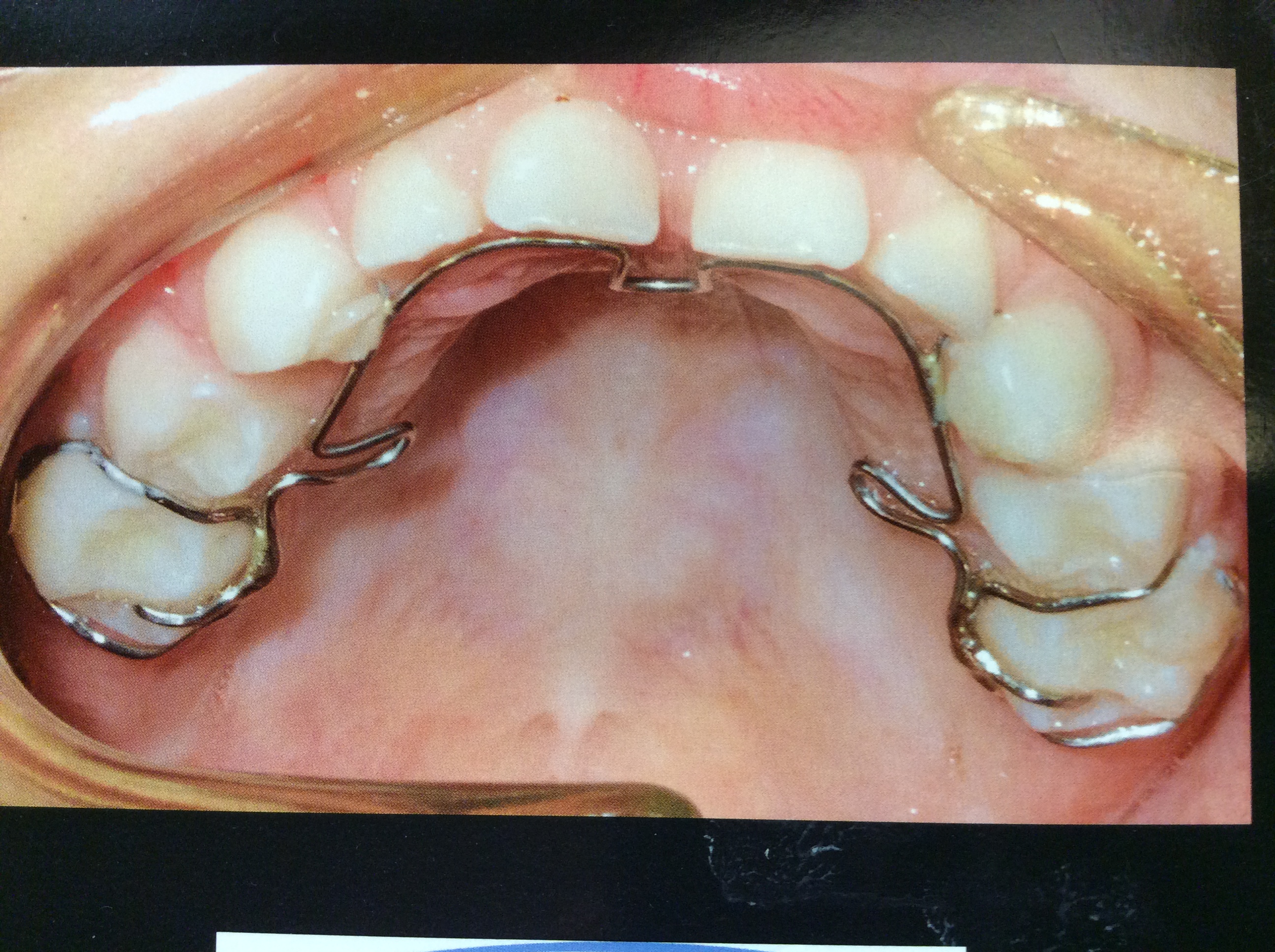
This methodology was invented by Dr. George B. Crozat and may resemble the ALF in that it also uses wires on the inside of the mouth. Designs vary much greater depending on the practitioner. The wires are also thicker, making teeth movement by the actual appliance much easier and independent of the tongue. It therefore relies less on function to correct structural problems. It is also a lot more robust and durable than the ALF. Facemask hooks can be added to the Crozat to help develop the upper jaw forward if it is deficient.
Case 1
Case 2
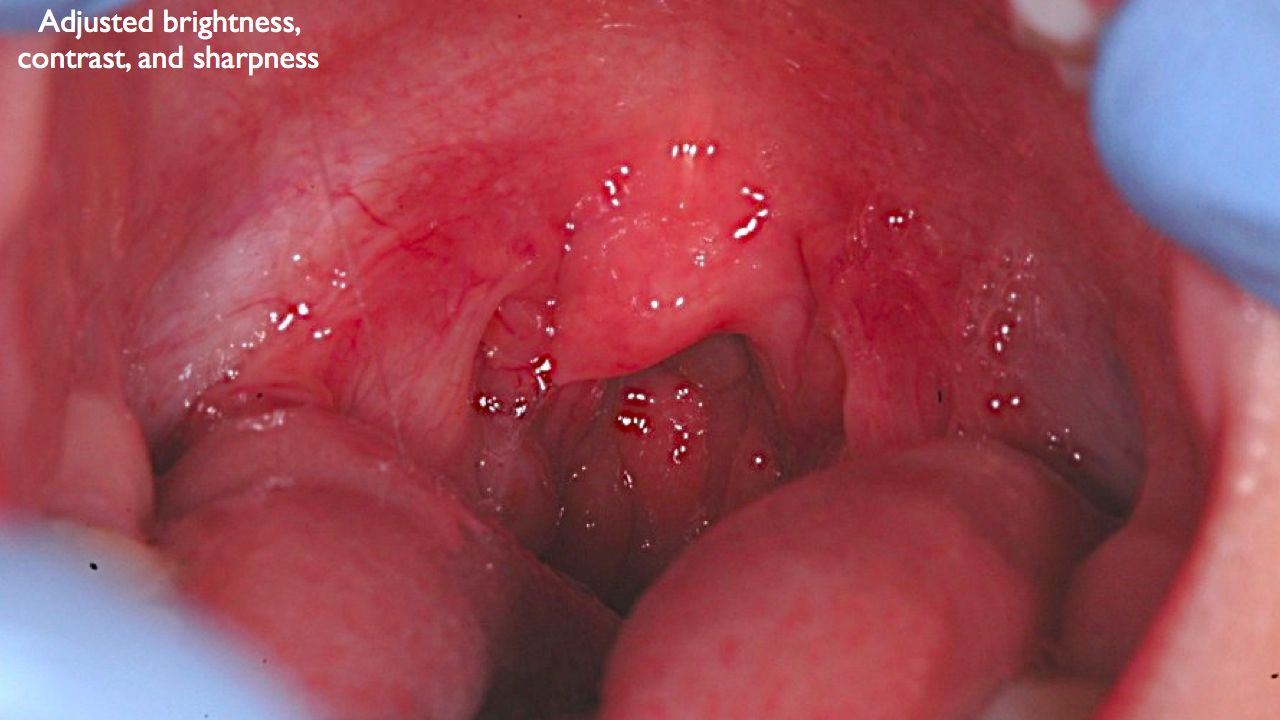
Crozat in the primary Dentition: 3 Yr Old child presents with snoring, large tonsils and adenoids, bedwetting, sleep apnea, allergies, reflux, deep bite, dental crowding resulting from under development of both upper and lower jaws. Goal of Crozat therapy to laterally expand both jaws, reverse the deep bite, espablish good spacing between baby teeth, encourage forward growth of the face, eliminate sleep apnea, allergies and reflux.